Thepainisreal.
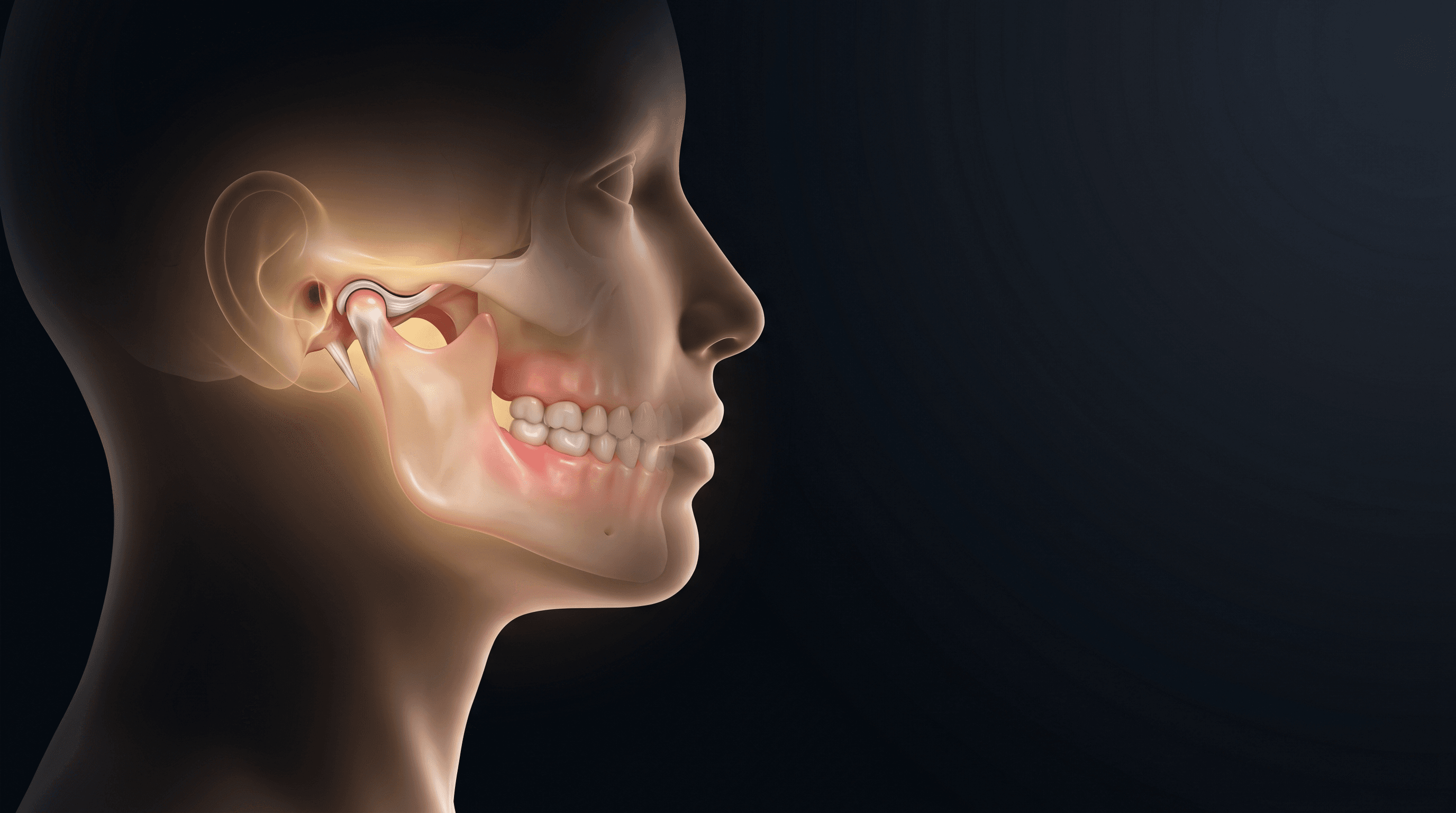
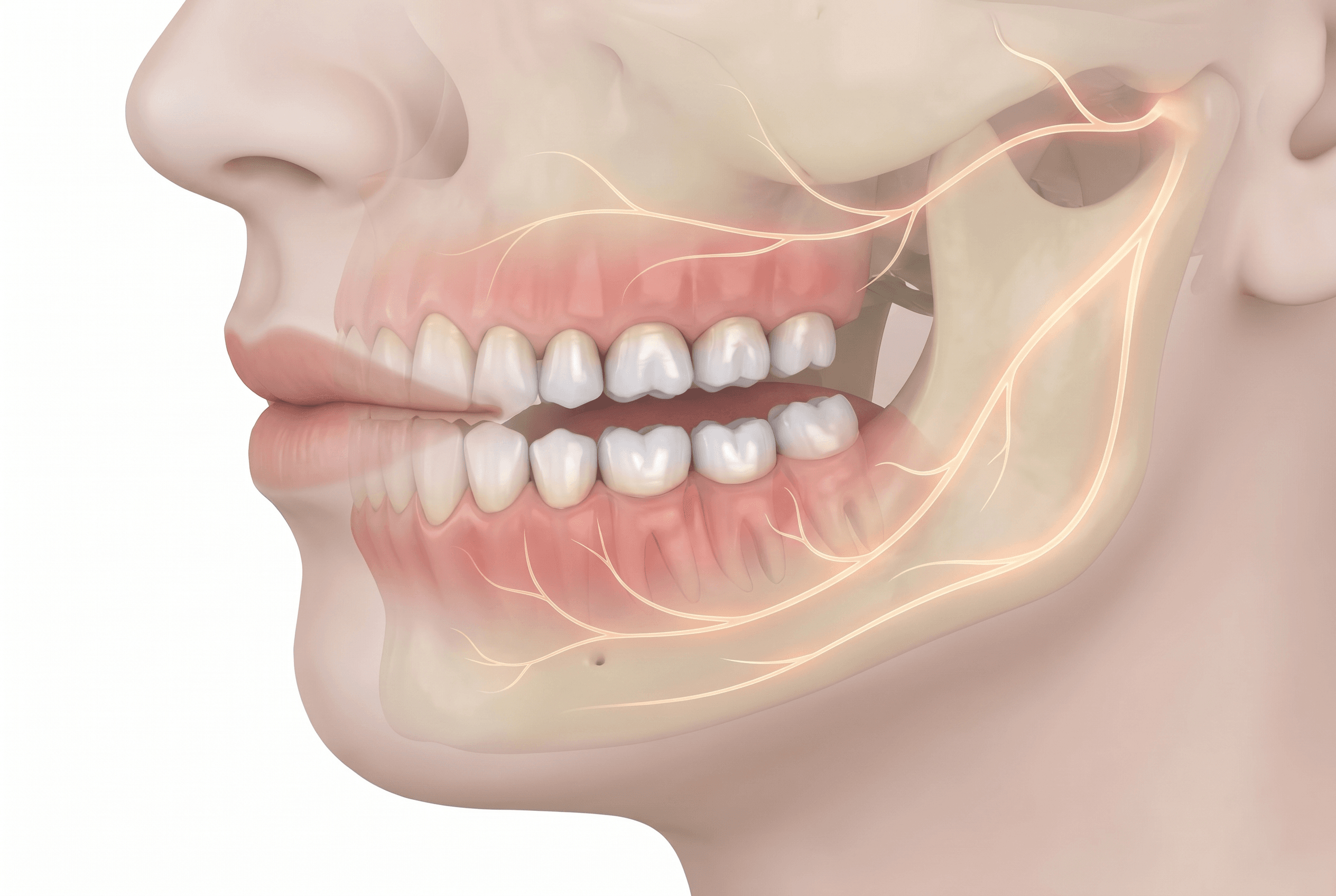
Jaw that clicks or locks. Headaches. Ear pain. A bite that feels off. TMJ disorders are easy to dismiss — but the ache has a physical cause: a small cushioning disc inside the joint has slipped out of place.
If you have jaw pain, clicking, popping, headaches, ear pressure, or limited opening, it's likely been misdiagnosed for years before someone connected it to bite mechanics. Most patients who find us have already seen a physician, a neurologist, or an ENT specialist, and nothing has been resolved. The problem lies at the intersection of dentistry and medicine, and very few practices are equipped to evaluate both sides.
We approach TMJ disorders the way a specialty clinic should: with a thorough history, a physical examination of the joint and masticatory muscles, and CBCT imaging that shows the joint in three dimensions. That imaging, taken with our iCAT FLX, reveals the bony architecture of the condyle, the degree of joint space narrowing, and any degenerative changes that would shift the treatment plan. What cannot be seen on a flat panoramic X-ray becomes visible. Decisions get better from there.
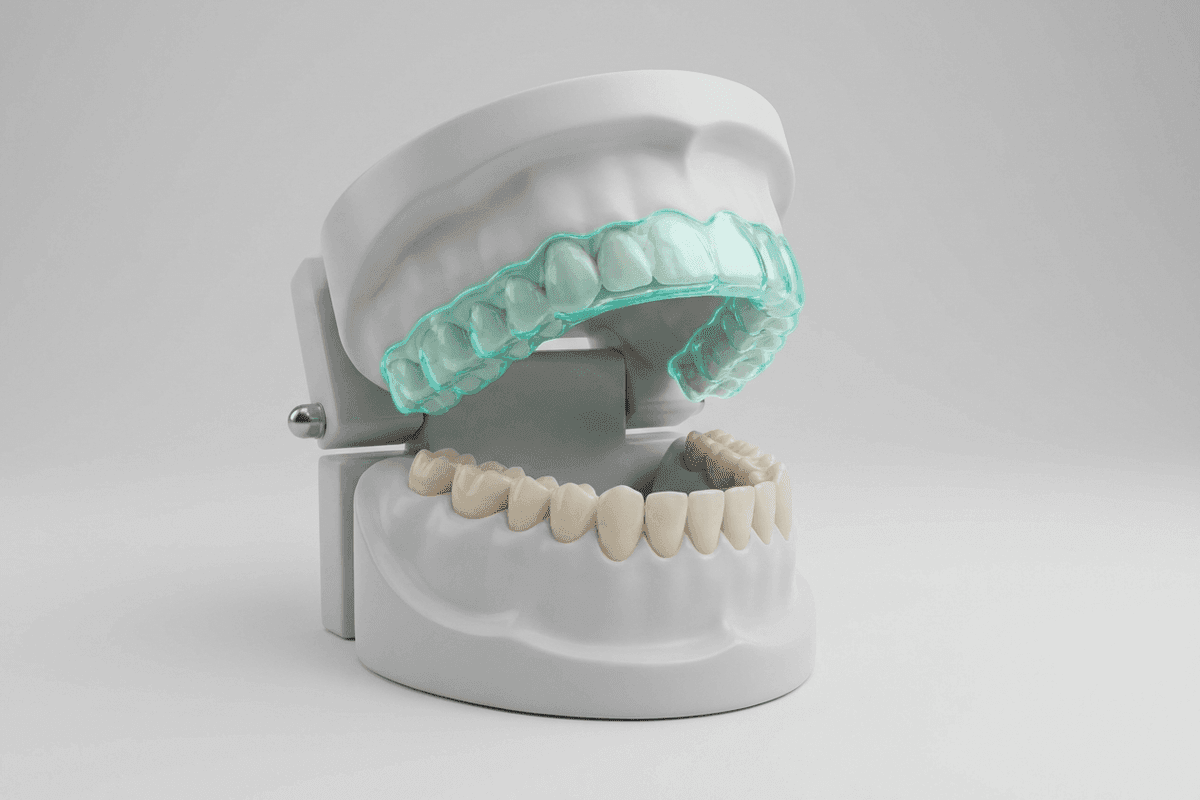
Treatment is always conservative first. Splint therapy — a precision-fit occlusal appliance worn during sleep, during the day, or both — reduces destructive joint loading and allows the tissues a chance to recover. Where the bite is contributing to the dysfunction, bite-equilibration addresses the root mechanical problem rather than masking it. Physical therapy and trigger-point work are often part of the same episode of care.
Surgery is a last resort, one we discuss candidly when we reach the limits of conservative management, but something most patients never need. Our goal is pain relief, jaw mobility, and a lasting result, not a dependency on a device.
How we evaluate.
01 · How we evaluate
Comprehensive bite analysis, jaw-joint imaging via 3D Cone Beam CT, muscle palpation, and a careful review of headache, ear, and sleep symptoms. Most TMJ cases are misdiagnosed as ear infections or tension headaches first.
How we treat.
02 · How we treat
Custom splint therapy, bite equilibration, physical therapy coordination, and targeted muscle work. We avoid surgical intervention except as a last resort and have not had to refer for surgery in the majority of our cases.
What patients tell us.
03 · What patients tell us
Most TMJ patients have been to multiple practices before us. The shared experience: someone is finally listening to the whole symptom picture, not just the part of it that's in the mouth.