Dental Practice · Periodontal & Surgical
Periodontal Treatment
Active treatment of gum disease — including laser-assisted therapy where indicated.
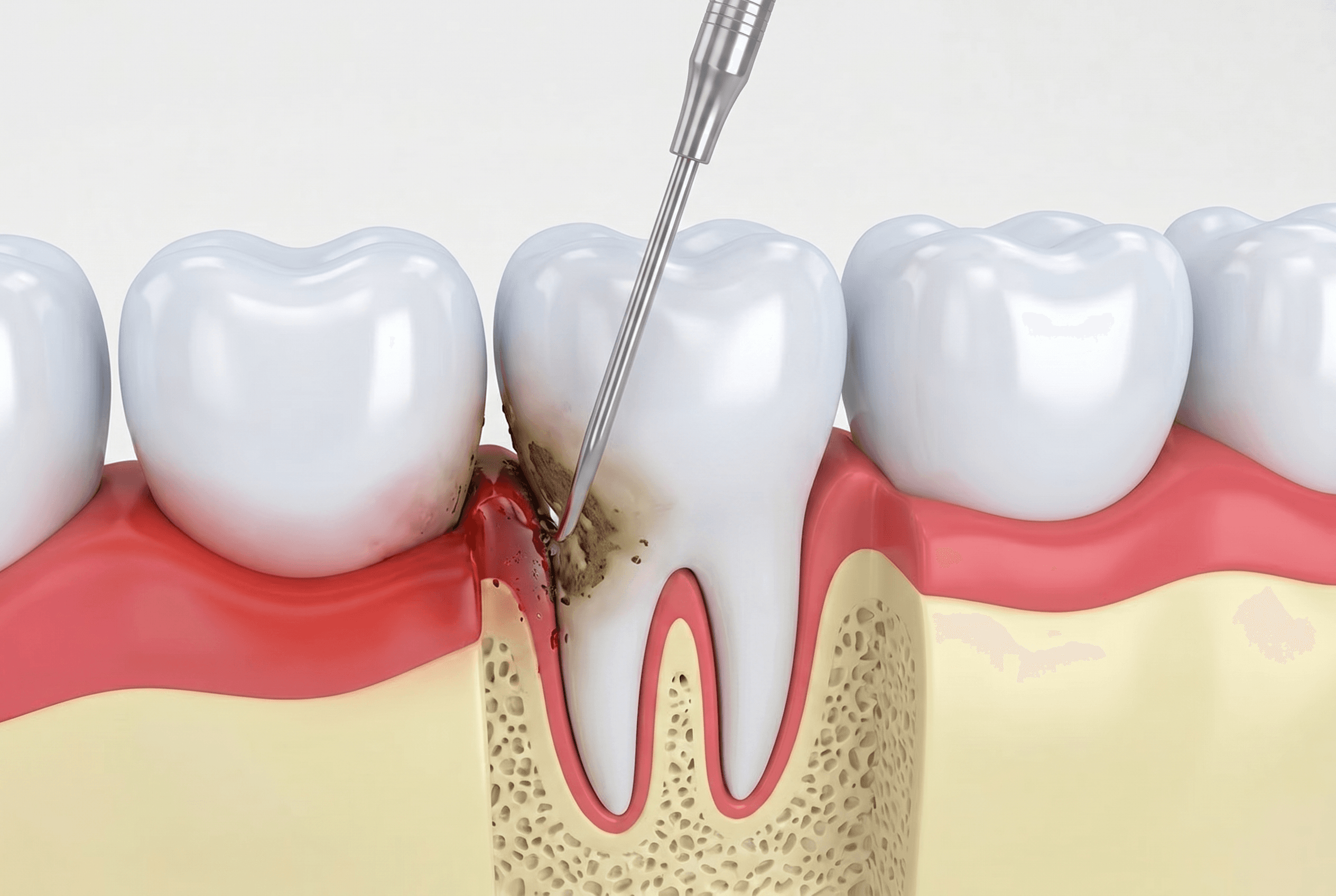
Periodontal disease is a chronic bacterial infection of the gum tissue and supporting bone around the teeth. It begins as gingivitis, which is inflammation without structural damage, reversible with improved hygiene and a cleaning, and progresses to periodontitis when the bacterial burden persists long enough to trigger bone resorption. The loss of bone that supports the teeth is not reversible. Managing periodontal disease is about arresting the progression, not restoring what has already been lost. The disease is widespread and underdiagnosed. A large portion of adults over thirty have some degree of periodontal involvement, and many of them do not know it. Periodontitis is frequently painless until it is advanced. The probing that happens at a comprehensive exam and at regular hygiene visits is the only way to detect it reliably. We screen at every cleaning visit. When we find pocket depths and bone loss consistent with periodontitis, we treat it directly rather than monitoring it through cleaning-only appointments. Active treatment begins with scaling and root planing: thorough removal of calculus and bacterial biofilm from root surfaces below the gum margin, under local anesthesia, one quadrant at a time. For infected pockets around teeth or implants, laser-assisted decontamination with our diode laser reaches areas that instruments alone cannot adequately address. After active treatment, we schedule the patient on a periodontal maintenance program — typically every three to four months rather than the standard six-month recall. The maintenance interval is based on individual risk, disease severity, and tissue response, not a fixed standard. Periodontal disease can be controlled with consistent maintenance; it progresses reliably without it.
Also in periodontal & surgical
Related services
Crown Lengthening
Surgical exposure of additional tooth structure for restorative or cosmetic reasons.
Gingivectomy
Soft-tissue contouring for periodontal pockets, hyperplasia, or cosmetic shaping.
Frenectomy
Release of restrictive frenum attachments: lip-tie, tongue-tie, or labial frenum.
Alveoloplasty
Surgical smoothing and reshaping of the bony ridge after extractions.